Why “Zero Calcium” Does Not Always Mean “Zero Plaque”
As a preventive cardiologist, one of the most common questions I hear is:
“My calcium score is zero. Does that mean my arteries are completely clean?”
The short answer is:
Not necessarily.
Coronary artery calcium (CAC) scoring has revolutionized cardiovascular risk assessment. It is fast, inexpensive, low-radiation, and supported by multiple guidelines as an effective tool for refining cardiovascular risk and guiding statin therapy decisions.
However, CAC has one important limitation:
It only detects calcified plaque.
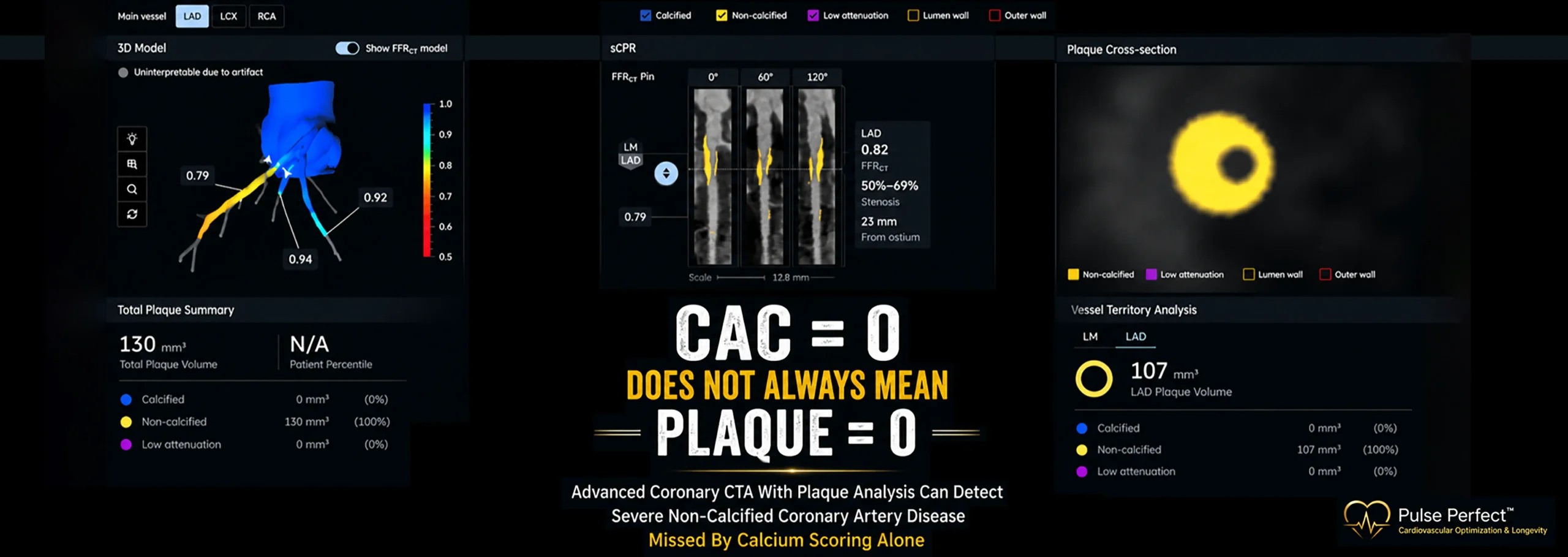
It does not detect soft plaque, non-calcified plaque, low-density plaque, plaque burden, or many of the high-risk plaque characteristics associated with future heart attack risk.
This is where Coronary CT Angiography (CCTA) with advanced plaque analysis provides a fundamentally different level of information.
What Does a Calcium Score Actually Measure?
A coronary calcium score quantifies the amount of calcified plaque within the coronary arteries.
A higher calcium score generally indicates a higher burden of coronary atherosclerosis and a greater future cardiovascular risk.
A score of zero is reassuring and associated with a lower short-term cardiovascular risk compared with individuals who have measurable coronary calcium.
However, a calcium score of zero does not mean the absence of atherosclerosis.
It simply means there is no detectable calcified plaque.
The Evidence: Zero Calcium Does Not Always Mean Zero Plaque
Large contemporary studies have demonstrated that coronary plaque may exist even when the calcium score is zero.
The Swedish Cardiopulmonary BioImage Study (SCAPIS), which evaluated over 30,000 middle-aged adults using coronary CTA, found that approximately 5.5% of individuals with a calcium score of zero still had coronary atherosclerosis, and a smaller subset had significant coronary artery narrowing.
Similarly, the Miami Heart Study demonstrated that approximately 16% of individuals with CAC = 0 had coronary plaque detected by coronary CTA, despite having no detectable coronary calcium.
These findings reinforce an important clinical reality:
Coronary plaque often begins as soft, non-calcified plaque long before calcium develops.
By the time calcium becomes visible, the disease process may have been present for years.
Why Coronary CTA Is Different
Coronary CTA allows us to visualize the artery wall itself rather than simply measuring calcium deposits.
In addition to identifying calcified plaque, coronary CTA can detect:
- Non-calcified plaque (soft plaque)
- Mixed plaque
- Total plaque burden
- Plaque location
- Degree of arterial narrowing
- High-risk plaque characteristics
- Functional significance when combined with technologies such as FFR-CT
This provides a much more comprehensive assessment of coronary artery disease.
Instead of asking:
“Is calcium present?”
Coronary CTA asks:
“Is coronary artery disease present?”
The Importance of Low-Attenuation Plaque
One of the most important advances in preventive cardiology has been the recognition that not all plaque carries the same risk.
Studies from the SCOT-HEART trial demonstrated that low-attenuation plaque burden was among the strongest predictors of future myocardial infarction, even after accounting for traditional risk factors, coronary calcium score, and stenosis severity.
Low-attenuation plaque is believed to represent lipid-rich, biologically active plaque that may be more vulnerable to rupture.
In many cases, these high-risk plaques may be present before substantial calcification develops.
In other words:
The plaque most likely to cause a future heart attack may not be the plaque seen on a calcium score.
What Do Current Guidelines Say?
The 2019 ACC/AHA Primary Prevention Guidelines support coronary calcium scoring to refine cardiovascular risk assessment and assist with statin decision-making.
The 2021 AHA/ACC Chest Pain Guidelines recognize coronary CTA as a highly effective tool for diagnosing coronary artery disease and improving risk stratification.
These guidelines acknowledge that coronary CTA provides substantially more anatomical information than calcium scoring alone.
Coronary Calcium Score vs Coronary CTA
Calcium Score Answers:
- Has plaque calcified?
- What is the burden of calcified plaque?
- What is the estimated future cardiovascular risk?
Coronary CTA Answers:
- Is plaque present?
- What type of plaque is present?
- How much plaque is present?
- Is there low-density plaque?
- Is there high-risk plaque?
- Is there obstructive disease?
- Is the disease progressing?
These are fundamentally different questions.
Why This Matters for Preventive Cardiology
Historically, cardiovascular medicine focused on identifying disease after symptoms developed.
Modern preventive cardiology focuses on identifying disease before symptoms occur.
The goal is not simply to find blockages.
The goal is to understand the biology of atherosclerosis early enough to alter its trajectory.
For selected individuals, including those with: strong family history of premature heart disease, high Lipoprotein(a), diabetes or prediabetes, south asian ancestry, metabolic syndrome, and high-performance executives seeking precision health optimization
Coronary CTA with plaque analysis helps provide actionable information that a calcium score alone cannot.
My Clinical Perspective
I still utilize coronary calcium scoring regularly because it remains a valuable and evidence-based tool.
However, when the objective is precision cardiovascular prevention, coronary CTA with advanced plaque analysis often provides a much more complete picture of coronary health.
The future of preventive cardiology is moving beyond simply asking whether calcium is present.
The future is understanding:
How much plaque exists?
What type of plaque exists?
Whether that plaque is stable or at high risk.
The earlier we identify atherosclerosis, the greater our opportunity to prevent the first heart attack rather than react after it occurs.
At Pulse Perfect, our philosophy is simple:
Screen Earlier. Optimize Aggressively. Perform Better. Live Longer.
KEY REFERENCES :
- SCAPIS (Swedish Cardiopulmonary BioImage Study): Prevalence of Subclinical Coronary Atherosclerosis in the General Population.
- Miami Heart Study: Coronary Atherosclerosis Among Asymptomatic Adults With CAC = 0.
- SCOT-HEART Trial: Low-Attenuation Plaque Burden and Future Risk of Myocardial Infarction.
- 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease.
- 2021 AHA/ACC Guideline for the Evaluation and Diagnosis of Chest Pain.