Coronary Artery Disease Care
Advanced Coronary Artery Disease Care & Early Risk Detection
Heart Attack Prevention Through Precision Cardiology
No symptoms · No warning signs. No indication that dangerous plaque has been building for years.
Until the first symptom is a major cardiac event.
#1
Coronary artery disease is the leading cause of death worldwide
49%
Of asymptomatic individuals found to have coronary plaque
(JACC 2022)
80%
Of people with prior heart attack had no idea they had CAD
(JAMA 2015)
0
Symptoms needed to qualify for advanced CAD detection at Pulse Perfect
Understanding the condition
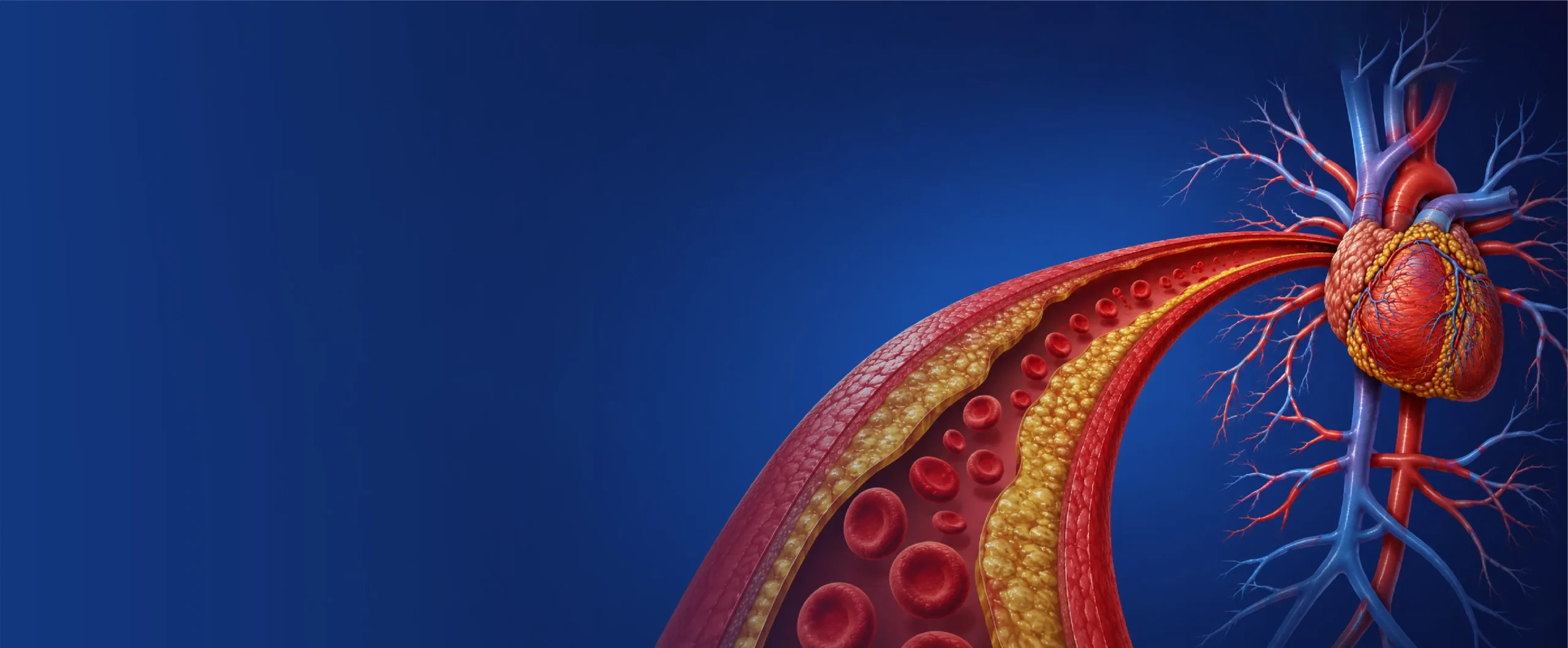
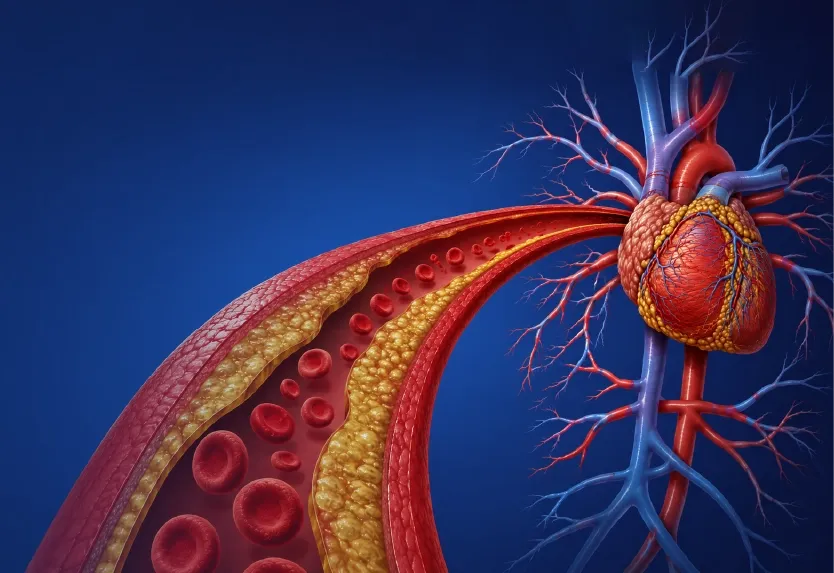
What is coronary artery disease?
CAD occurs when plaque accumulates inside the arteries supplying blood to the heart. Silently and gradually narrowing them over decades, before any symptom appears.
Coronary plaque is made of
- Cholesterol — the primary building block of arterial plaque
- Calcium — calcified deposits that harden with age
- Inflammatory material — immune cells trapped in arterial walls
- Fat — lipid-laden foam cells accelerating plaque growth
Over decades, this plaque narrows the arteries and restricts blood flow to the heart, often with no warning.
As plaque builds, risk accumulates for
- Heart attack — when a plaque ruptures and blocks blood flow
- Stroke — from clots originating in diseased coronary vessels
- Reduced blood flow — causing angina and limited exercise capacity
- Long-term cardiac damage — progressive loss of heart function
The challenge: CAD often develops quietly over 20–30 years before any symptom appears. Traditional cardiology rarely investigates until symptoms arrive.
The silent killer
Most people with CAD don't know they have it
Coronary artery disease earns its name. Exercise, healthy habits, and routine checkups provide no guarantee, because standard evaluations don’t look for plaque.
They exercise regularly
Physical fitness reduces risk, but does not eliminate it. Plaque accumulation can progress even in active individuals with excellent cardiovascular performance.
They pass annual physicals
Standard checkups EKGs, basic cholesterol panels, blood pressure readings, are not designed to detect early plaque. A clean report is not the same as a clear artery.
They feel completely well
The first symptom of CAD for many people is a heart attack, sudden chest pain, or a major cardiac event. The absence of symptoms does not guarantee the absence of disease.
If you experience chest pain or pressure, shortness of breath at rest, pain radiating to the jaw or arm, or sudden dizziness, seek emergency medical attention immediately. The information on this page is for individuals seeking proactive cardiovascular evaluation, not emergency care.
Understanding your risk
Some risks are genetic and some are modifiable
Knowing which category your risk factors fall into, and how they interact, is the foundation of a meaningful prevention strategy.
CANNOT CONTROL
FIxed Risk Factors
- Age — cardiovascular risk increases significantly after 45 in men and 55 in women
- Family history of heart disease, especially early-onset (before 55 in men, 65 in women)
- HDL and triglycerides, a useful context, but incomplete without particle data
- Elevated Lipoprotein(a) [Lp(a)] — inherited and largely unresponsive to lifestyle alone
Fixed risks cannot be eliminated, but they can be detected early, monitored precisely, and meaningfully offset through advanced prevention.
CAN INFLUENCE
Modifiable Risk Factors
- High blood pressure : managed through lifestyle, monitoring, and medication precision
- Elevated ApoB and LDL : addressable with advanced lipid strategies beyond standard statins
- Diabetes and insulin resistance : metabolic optimization significantly reduces risk
- Chronic stress : nervous system regulation and recovery strategies lower cardiovascular load
- Poor sleep quality : sleep architecture directly affects arterial inflammation and repair
- Visceral fat and physical inactivity :VO₂ max improvement is the strongest longevity lever
Sustained pressure damages arterial walls, accelerating plaque formation and long-term coronary disease risk.
The absence of symptoms does not mean the absence of damage. Early evaluation changes long-term outcomes.
The gap in traditional care
Standard testing often detects CAD too late
Routine evaluations are designed to manage existing disease, not to detect it before it becomes dangerous. In most systems, advanced imaging requires symptoms first.
Standard evaluation typically includes
- Basic cholesterol panel misses ApoB, Lp(a), particle size, and plaque burden
- Resting EKG which is normal in most patients with early-stage CAD
- Occasional blood pressure readings with no insight into pattern, timing, or stress response
- Advanced imaging which is typically only approved after symptoms appear or a stress test fails
What’s missing from the standard picture
- Coronary plaque burden which reveals what's actually inside the arteries right now
- Early arterial inflammation which accelerates plaque growth silently.
- Plaque composition, soft vs calcified determines rupture risk
- Advanced lipid particle data. ApoB and Lp(a) that predict events standard LDL misses
At Pulse Perfect, we focus on identifying risk before symptoms appear, not after the first cardiac event.
Our advanced diagnostic approach
Detecting coronary disease before symptoms appear
Every diagnostic tool below is available without symptom threshold, insurance pre-authorization, or referral delays at Pulse Perfect.
Gold standard imaging
Coronary CT Angiography (CCTA), seeing what standard testing cannot
Gold standard imaging
Coronary CT Angiography (CCTA), seeing what standard testing cannot
CCTA is advanced cardiac imaging that directly visualizes the coronary arteries — detecting both calcified and soft plaque, arterial narrowing, and early coronary artery disease often years before any symptom or abnormal stress test. Unlike routine stress testing, which identifies reduced blood flow only after arteries are significantly narrowed, CCTA finds plaque at the formation stage.
Calcified plaque
Soft / vulnerable plaque
Arterial narrowing
Early arterial disease
No symptoms required
Coronary Artery Calcium (CAC) scoring
Measures calcium deposits within the coronary arteries, converting abstract cardiovascular risk into a concrete, measurable number.
- Predicts future heart attack risk with strong precision
- Identifies hidden plaque burden in asymptomatic patients
- Guides intensity of prevention strategy
Advanced Lipid & Inflammatory Testing
Two people with identical LDL can carry very different cardiovascular risk. Advanced biomarkers reveal what standard panels miss.
- ApoB : the true measure of plaque-forming particle load
- Lp(a): inherited risk affecting 1 in 5 people
- hs-CRP and metabolic inflammatory markers

Performance & Longevity Testing
Cardiovascular health is more than the absence of disease, it’s the presence of resilience and long-term physical capacity.
- VO₂ max analysis, the strongest predictor of longevity
- DEXA body composition and metabolic profiling
- Biological age and nutrigenomic assessment
Your personalized CAD blueprint
A long-term prevention strategy built around you
Following diagnostics, we build a comprehensive, personalized cardiovascular strategy and not a generic management plan.
The goal is to change the trajectory of disease early, not manage its progression.
1
Plaque burden and risk quantification
CCTA and CAC scoring to establish a precise baseline, turning “I might be at risk” into data-driven clarity.
2
Advanced biomarker and metabolic analysis
ApoB, Lp(a), inflammatory markers, VO₂ max, biological age, and metabolic profiling to complete the risk picture
3
Personalized cardiovascular optimization strategy
Nutrition, exercise prescription, sleep and stress optimization, and medication management when clinically appropriate
4
Year-round physician partnership
Quarterly goals, continuous monitoring, and real-time strategy adjustments, not a one-time report with no follow-through
Your first visit includes
- Comprehensive 60-minute consultation with Dr. Patel
- Same-day electrocardiogram (EKG)
- Personalized cardiovascular risk blueprint
- CAD risk stratification and prevention roadmap
- Direct phone access to Dr. Patel for follow-up
No referrals
No Insurance
No rushed visits
Evidence-based treatment & prevention
Medication and lifestyle work together and not separately
Sustainable CAD prevention requires a system-level approach. When clinically appropriate, we integrate precision pharmacology with comprehensive lifestyle optimization.
Statin therapy optimization
Right molecule, right dose, right timing, statin regimens calibrated to your ApoB target and plaque burden, not a population average
Advanced lipid-lowering therapies
PCSK9 inhibitors, inclisiran, bempedoic acid, and ezetimibe, for aggressive LDL and ApoB reduction beyond statin monotherapy
Blood pressure optimization
24-hour ABPM, medication timing precision, and lifestyle integration to protect arterial health continuously, not just in-office
VO₂ max improvement programme
The single most powerful intervention for longevity — personalized exercise prescription to measurably improve cardiovascular fitness
Sleep and stress optimization
Sleep architecture and nervous system regulation directly influence plaque progression and are addressed as primary cardiovascular interventions
Nutrition & metabolic optimization
Nutrigenomic-informed dietary strategy, metabolic profiling, and body composition management to address the metabolic drivers of CAD
The Pulse Perfect difference
Beyond traditional cardiology
Traditional Cardiology
Symptom-driven. Reactive. Fragmented.
- Short appointments focused on managing presenting symptoms
- Advanced imaging only after symptoms or stress test failure
- No continuity. Limited physician access between annual visits
- Reactive treatment. Waits for disease progression to intensify care
Pulse Perfect
Proactive. Precise. Year-round.
- Advanced imaging and biomarkers available without symptoms
- Precision risk assessment of plaque, particles, and genetics
- Year-round physician oversight with direct access to Dr. Patel
- Personalized prevention strategy. No one-size-fits-all protocols
When to seek Evaluation
Symptoms should never be ignored
Know the difference between an emergency requiring immediate attention and the proactive evaluation this programme is designed for.
Seek emergency care immediately
Do not wait. Call emergency services now if you experience
- Chest pain, pressure, or tightness
- Shortness of breath at rest or with minimal activity
- Pain radiating to the jaw, left arm, shoulder, or back
- Sudden dizziness, fainting, or loss of consciousness
Consider proactive CAD evaluation if
You’re ready to understand your risk before symptoms appear
- You have multiple cardiovascular risk factors
- You have a strong family history of heart disease or early cardiac events
- You've been told your reports are "normal" but still want real clarity
- You're focused on longevity, prevention, and long-term performance
Who this is for
This is for you if
- You have a family history of heart disease, heart attack, or early cardiac death
- You have elevated cholesterol, blood pressure, or known lipid abnormalities
- You've been told your cholesterol is "normal" but still want deeper cardiovascular clarity
- You want advanced CAD screening and not just a standard annual physical
- You've been told your reports are "normal" but still want deeper cardiovascular clarity
- You're 35+ and focused on long-term prevention, longevity, and performance
- You want a physician partner and not an annual appointment with no continuity
Limited Availability
Don't Wait for Symptoms to Take
Your Health Seriously
The best time to address cardiovascular risk is before you feel it.
Our programme accepts a limited number of new patients each quarter to ensure the highest standard of personalised care.
Apply for a Longevity Consultation
Limited patients accepted · Concierge access · NYC & NJ
Common Questions
Everything You Need to Know
Answers to the most frequently asked questions about concierge preventive cardiology, our process, and what to expect from your PulsePerfect journey.
Can I have coronary artery disease without symptoms?
Yes. CAD often develops silently for years before symptoms appear.
What’s the difference between a calcium score and CCTA?
A CAC score measures calcified plaque burden and gives you a risk number. CCTA goes further, it visualises both calcified and soft (non-calcified) plaque, arterial narrowing, and early disease that a calcium score alone cannot detect. They are complementary tools.
Can coronary artery disease be prevented?
Early detection and aggressive risk optimization can significantly slow progression and reduce cardiovascular events.
Can coronary artery disease be reversed?.
You cannot completely reverse established coronary artery disease—plaque that’s calcified will remain. However, research shows that aggressive intervention can stabilize existing plaque (preventing rupture), stop disease progression, and in some cases modestly reduce plaque burden.
The key is catching disease early and implementing comprehensive prevention strategies. Dr. Patel’s approach focuses on preventing progression and optimizing your cardiovascular trajectory for decades to come.
How do I know if I have CAD if I feel fine?
Most people with CAD have no symptoms until plaque ruptures and causes a heart attack. The only way to know definitively is through advanced diagnostic testing such as coronary calcium scoring or CT angiography.
If you’re over 40 (men) or 50 (women) with any risk factors, you should know your calcium score. Don’t wait for symptoms—they often appear too late.
What’s the difference between a calcium score and coronary CT angiography?
Calcium Score (CAC): A quick, low-dose CT scan that measures only calcified plaque. It provides a risk score but does not visualize arteries in detail.
Coronary CT Angiography (CCTA): A comprehensive imaging study that visualizes all plaque (calcified and non-calcified) and shows the exact location and severity of blockages.
Dr. Patel’s Approach: We often start with calcium scoring. If results show significant plaque or high-risk features, we proceed to CCTA for complete evaluation.
Is advanced imaging necessary if my cholesterol is normal?
In some individuals, yes. Standard cholesterol testing may not fully reflect plaque burden or inherited cardiovascular risk.
Will my insurance cover advanced CAD testing?
Insurance typically covers testing only after symptoms appear or after a positive stress test. Proactive screening in asymptomatic individuals is often denied—even when medically appropriate.
Pulse Perfect’s concierge model operates outside insurance limitations to provide the testing you need when you need it—not when insurance finally approves it.
Consider: A 5-day hospital stay for a heart attack costs approximately $14,000. Preventing that event through early detection is priceless.
How is Pulse Perfect different from my current cardiologist?
Traditional cardiologists excel at managing acute cardiac events and established disease within insurance protocols.
Pulse Perfect prevents cardiac problems before they occur through:
- Year-long concierge access (not episodic visits)
- Advanced diagnostics unavailable in insurance-based practices (CCTA, VO₂ max, nutrigenomics)
- Quarterly optimization goals with continuous adjustments
- Direct cardiologist communication—no gatekeeping
How quickly can I start as a patient?
New consultations are typically available within 5–7 business days.
We prioritize urgent cardiovascular concerns and can often accommodate same-week appointments for Central New Jersey professionals.